Spinal Cord Injury (SCI)
Level of injury
Level of injury can be defined using two different anatomical methods:
Vertebral column
The level of injury could communicated relative to the vertebral column. For example one could say a spinal cord injury at T12 vertebral body.
Spinal cord level
Completeness
Completeness of the spinal cord injury refers to how much of the the spinal cord was damaged in the injury. For example, a “complete” spinal cord injury would injury the entire cross-section and no sensation would be able to come up the spinal cord and no motor would be able to be sent inferior of this section.
Functional Categories
Spinal cord injuries can be divided into two functional categories: tetraplegia and paraplegia2
Tetraplegia
Paraplegia
Anatomy
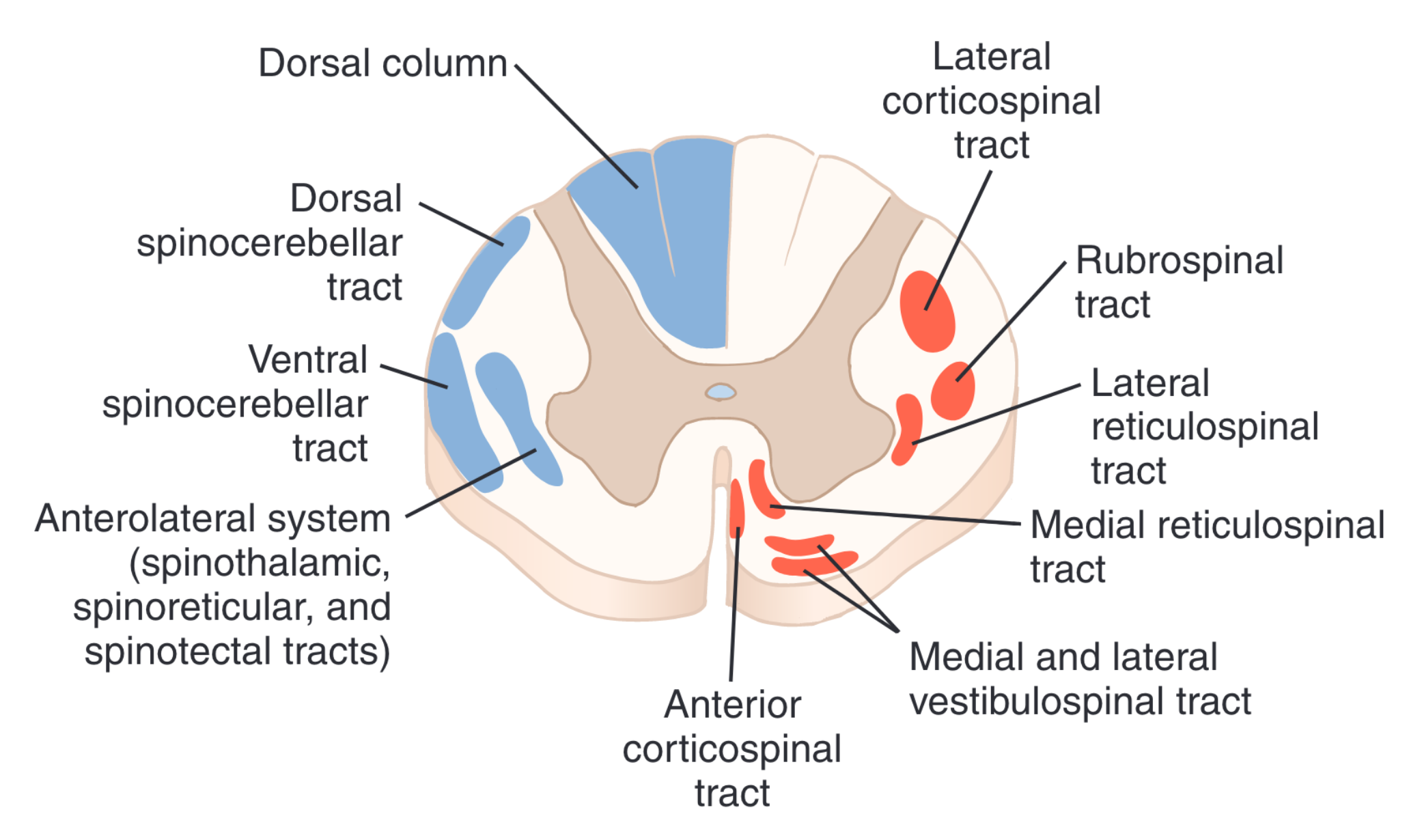
Read more about the Anatomy and function of the spinal cord.
Determining Lesion Level and Severity
It is important for clinicians to be able to determine lesion level and completeness in order to establish prognosis. The standardized method to assess this is the ISNCSCI.
Clinical Syndromes
- Clinical syndromes refer to common patterns in SCI presentations2.
- ~\(\frac{1}{5}\) of clinical presentations follow clinical SCI syndromes2.
Clinicians should use clinical syndromes to anticipate sensory and motor functions, which they can use for goal-setting, predicting outcomes, and guiding the plan of care (POC)2.
Brown-Sequard Syndrome
- Brown-Sequard Syndrome
- Generally due to penetration injuries
- Hemisection
Anterior Cord Syndrome
- Anterior Cord Syndrome
- Flexion injury (generally)2
- BIL Corticospinal tract damage
- BIL Spinothalamic tract damage
- DCML Preservation
Central Cord Syndrome
Cardiovascular complications
Disruptions of cardiovascular control following spinal cord injury are directly related to the level and degree of the injury3
Timing
Acute
“Immediately after a spinal cord injury, there is in almost all patients a sudden loss of the autonomic effect of the smooth muscle in the walls of the blood vessels, and as a result vasodilation occurs. The acute loss of sympathetic stimulation results in bradycardia. During the acute phase, the arterial hypotension (neurogenic shock) may be misinterpreted as loss of volume.”3
Peripheral Nerves
Vagus Nerve
- The vagus nerve is hypersensitive immediately after an injury3.
- This normally lasts for 2–3 weeks, but can last longer3.
- Treatment
- Implantation of a temporary or permanent pacemaker is required.
- Atropine should be available3
- Precautions:
- This can be a life-long problem in patients with high, complete injuries, whereas in patients with lower and/or incomplete injuries the situation may normalise after 4–5 weeks3
Complete Cervical
“complete cervical injury, the connection between the upper autonomic centres in the brain and the intermediolateral cell column at level T1–L2 of the spinal cord will be destroyed. Patients with cervical injuries have a higher risk of bradycardia (29 %), sudden unprovoked cardiac arrest (16 %) and conduction system disturbances, particularly in the first few weeks after the injury (5). Sudden death is not unusual either.”3
Injuries by Segments
| Level | Muscle Group |
|---|---|
| C5 | Elbow flexors |
| C6 | Wrist extensors |
| C7 | Elbow Extensors |
| C8 | Finger Flexors |
| T1 | 5th Finger Abductors |
| L2 | Hip flexors |
| L3 | Knee extensors |
| L4 | Ankle Dorsiflexors |
| L5 | Long Toe Extensors |
| S1 | Ankle plantarflexors |
| Segmental level | Transfers | Wheelchair |
|---|---|---|
| C1-4 | Mechanical lift | Power WC with head/chin/mouth control |
| C5 |
Dependint |
Manual WC with Plastic coated hand rims |
| C6 | Independent sliding board transfer | Manual WC with Plastic coated hand rims |
| C7/8 |
|
Manual WC with Plastic coated hand rims |
| T1 | Floor to Wheelchair | Independent |
| T4 | Sitting pivot | Independent |
| L3 | Standing pivot | Independent |
Clinical Presentation
Pain
- Bonica’s Managmenet of Pain ch40: Pain Following Spinal Cord InjuryballantyneBonicaManagementPain2019?
- Welzack Chapter 68 Pain Following Spinal Cord Injury4
Intervention
Stem Cells
- Paul video:
- one guy said that it significantly worsened pain and spasticity
- See “Systematic Review of Cell Therapy Efficacy in Human Chronic Spinal Cord Injury”5
Virtual Reality
Examination
Participation
QOL:
- Sickness Impact Profile 68 (SIP-68)